
News
A Porter doctor sees action in NYC hospital

I am an anesthesiologist at Porter Hospital in Middlebury, but I lived in New York City for over 20 years. When it became clear that the excellent work of Vermonters was turning our state into something of a COVID-19 success story, I volunteered late last month to go down and work in my old hometown. I was deployed for almost two weeks to a hospital in Queens, a very hard-hit part of the city.
The minute I arrived, I could feel the difference. At Employee Health, several people (sometimes with their masks off) approached the desk to talk about their positive tests or their worrisome symptoms. Alarmingly often, stretchers with masked or intubated patients were waiting at the elevators; even with my face covered, I was nervous walking by them. In late March, at the crest of the “wave,” whole departments were closed so that 85-90% of the hospital could be turned over to COVID patients, and four refrigerated trucks were brought in as makeshift morgues. “Everyone who lives nearby has lost someone,” a staff doctor told me.
The hospital sent me to work in Labor and Delivery, where an anesthesiologist is always needed but work is sporadic. This freed up one of their staff for more regular jobs. Of course, it also made it easier for me to avoid or manage any COVID exposure, since there are relatively few total emergencies in L&D, and all the pregnant women are tested for the virus. I breathed a little easier.
I began to hear about a patient (I’ll call her Jane) who had just returned to us from the Intensive Care Unit. She had come to the hospital almost five weeks earlier, 23-1/2 weeks pregnant and infected with COVID. Despite treatment, she deteriorated, and spent the next four weeks with a breathing tube. She fought off the virus, but then developed a secondary infection with an antibiotic-resistant bacterium. Several times, the ICU tried to extubate her — remove the breathing tube. Each time, they failed. The whole team feared she wouldn’t make it. Finally, in a last-ditch effort to save her, they decided to deliver her 28-week, 2-pound infant by C-section. In what must have felt like a double miracle, the very premature infant came out strong and crying, and almost immediately Jane began to improve. When I arrived she had been extubated and breathing on her own for several days.
The PPE (personal protective equipment) situation in the hospital was…adequate. There seemed to be no clear protocols for what we should wear, but most of us have developed a sense of that from looking into it ourselves. And happily, I saw no sign of the severe shortages we have all read about. There were still some compromises, though. We only received one N-95 mask per day, and the gowns the hospital supplied felt flimsy and too short. On the other hand, I was issued a good face shield, and there were surgeons’ hoods that covered most of my head and neck. More importantly, like all practitioners these days, I had gotten proactive. A colleague at Porter managed to find me an excellent P-100 respirator (stronger than the N-95), which I brought with me from Vermont. All in all, I felt safe enough.
This was put to the test on one of my first days, when a woman with an abruption — a severe, life-threatening disruption of the baby-nourishing placenta — needed an urgent C-section. We did not know her COVID status, and had to intubate her — one of the most dangerous procedures you can do with this virus. But, with our PPE close by, we were able to “don” it in time to get the baby delivered without delay. Afterwards I tried to be as meticulous as I could cleaning and disposing of my PPE — although, again, the hospital appeared to have no clear protocol for this. We all felt better when, a few hours later, the patient’s COVID test came back negative.
A few days after Jane was brought back to the ICU, she was still not thinking clearly, and an MRI showed she was bleeding around the edges of her brain. The consensus was that this was not necessarily serious — but no one knew why it was happening, either. Was the virus attacking the lining of the blood vessels, leading to clots and bleeding? As with every other COVID question — who is infectious; how long will we need to keep social distancing; what will the world look like in six months? — no one knows. In 2015, I worked on the Ebola outbreak in Africa; even though that disease was more dangerous, we understood it better. In that sense, dealing with coronavirus has actually been much harder.
Whenever a COVID patient was successfully discharged, there was a PA announcement, and the hospital played a snippet of Bill Withers’s “Lean on Me.” It began to happen so often that, toward the middle of my stint, I heard staff members complaining they were tired of the song. I also heard nurses talking about finally being able to schedule vacations. The hospital’s COVID “census” had declined by 30% in the week before I arrived, and they were about to give us back the half of Labor and Delivery they had commandeered as an extra COVID ward. Outside, we were down to “only” two morgue trucks. I even heard the nurses joking around: in nine months, seeing as everyone is inside right now, they are expecting a surge of babies, and one of them thought that “Korona” and “Kwarantine” might make nice names.
At this point, I caught myself starting to commit a mental error: half starting to believe that the disease itself had gotten less serious, when all that had actually happened was that patient numbers had finally declined enough to start being manageable. The stories brought me back to reality. One of our patients had a mild case of COVID, but her mother was in the ICU in Manhattan and her husband felt sick but was afraid to get tested because he was an undocumented immigrant. One of the doctors knew a nurse who, many years ago, adopted the four children of a patient who died. Now the nurse’s husband had succumbed to COVID, and she herself was intubated in the ICU. What will happen to those children?
The story that affected me most came on my second Monday. The staff was gathered around a doctor I had not met before, a man with a kind, open face who was obviously beloved. He had been on a two-week break because the virus had sickened and killed first one and then the other of his parents. How he managed to be back at work I do not know.
Toward the end of my assignment, the hospital was offering antibody tests, so — despite questions about the tests’ reliability — I got one. Negative — no antibodies. Darn. I had half-hoped that some mild exposure I didn’t know about had given me resistance without actually making me sick. Some of the nurses with positive results were celebrating, but I had to go back to the mild anxiety of the “at risk.”
And then my last day, it happened. I went in to see a woman who needed a C-section (healthy, no symptoms) and carelessly neglected to put on my full PPE. A few hours later, there was a buzz at the nurse’s station: The patient had tested positive. My exposure qualified as “low risk” — if I weren’t leaving the hospital, I would most likely still have been allowed to come in to work. I wasn’t too worried for myself. But it meant I would have to be extra careful about any contacts with others until I tested negative the following week. Needless to say, I felt like an idiot.
But Jane was going home. Like so many COVID patients, she had had a collection of strange findings — that bleeding around her brain, a falling platelet level, some lingering confusion after weeks of sedation. But all of them had stabilized enough to let her go back to her devoted husband and three older kids. The staff, who had been fighting this war for so much longer than I had and who had seen so many people die, were planning a celebration. They were all — we are all — looking toward a future that none of us can quite imagine yet. We need a few success stories like this to carry us through.
Click here to read the story of a Weybridge man who caught the disease.
More News
News
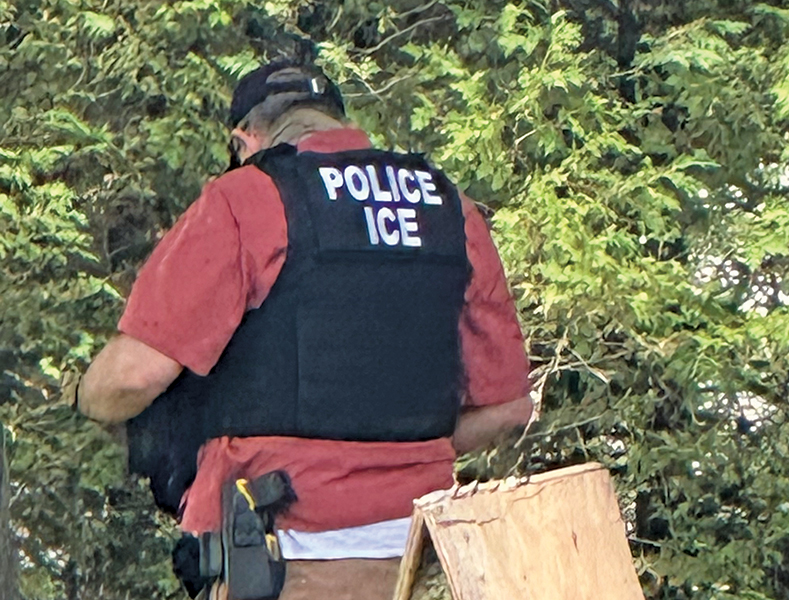
Updated: ICE arrests two men in Cornwall on Saturday
In a sweep of Immigration and Customs Enforcements action over the past few days, federal … (read more)
News

Profiles in Community: AlwaysEvolving Details takes auto cleaning to new heights
“I got sick of destroying vehicles and wanted to make them clean and new instead.” — Devin … (read more)
News
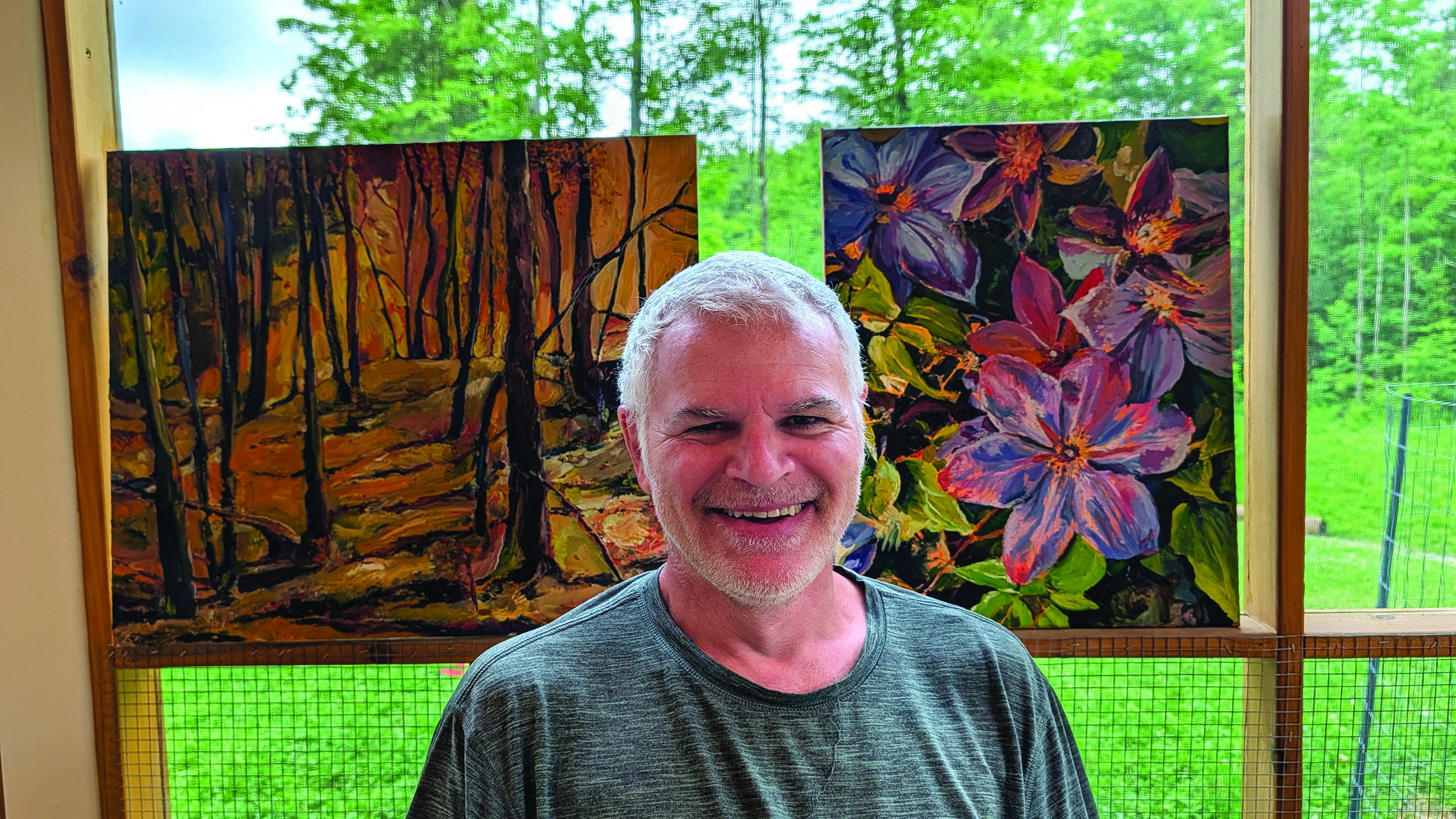
Profiles in Communty: Former art therapist now paints his own art catharsis
“I always dreamed of having a dedicated studio, but I seem to gravitate towards making the … (read more)





